


The Utstein Formula for Survival depicts the three components essential to improving survival from sudden cardiac arrest – medical science, educational efficiency, and local implementation. While equally weighted from a mathematical perspective, only recently has education stepped into the spotlight with its fellow factors to exact its importance in the formula for survival. This paradigm shift is important. In an area where education has traditionally been a second consideration, it is now being given the attention it deserves. This newfound reputation is heavily attributed to the 2018 publication of the American Heart Association’s scientific statement: Educational Strategies to Improve Outcomes from Cardiac Arrest.
Medical Science x Educational Efficiency x Local Implementation = Survival
(Utstein Formula For Survival)
What is educational efficiency? How do we elevate resuscitation education to a standard that will not only improve performance, but maintain it over time? The answer is in the design, instructional design that is. Simply put: how do you best teach resuscitation education in a quality improvement model?
As the statement reflects, at the cornerstone of design are instructional strategies and educational philosophy elements such as mastery learning and deliberate practice, spaced learning, feedback and debriefing, contextualization, and assessment. Enhancing instructional design in the context of these elements can improve educational outcomes, patient outcomes, and ultimately survival after cardiac arrest.1
Talking design is one thing but walking design, in regard to the application of quality resuscitation education, is another. It challenges traditional learning environments, puts feasibility on edge, and requires a shift in culture that is not for the faint of heart (pun intended). But, it can improve outcomes. That’s why RQI felt it was imperative to raise the bar in resuscitation education. Let’s take a look at how.
RQI Design Elements
Mastery Learning & Deliberate Practice, activities that have been specifically designed to improve the current level of performance to demonstrate a predefined level of competence for a specific skill.2
RQI Design Elements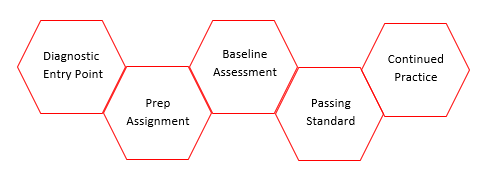
Low-Dose, High-Frequency, activities that are delivered in smaller doses with repetition over time for recall and memory consolidation.
RQI Design Elements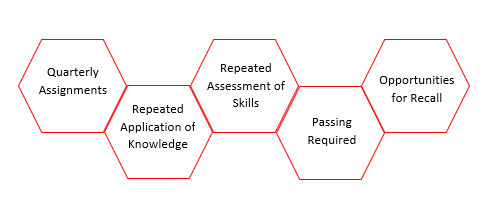
Feedback, information about the performance compared to a standard.3 & Debriefing, reflective evaluation of performance that includes feedback.4
RQI Design Elements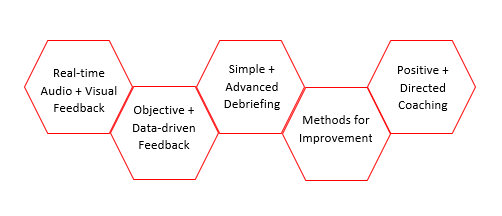
Contextual Learning, the applicability of training experiences to a real-word practice.1
RQI Design Elements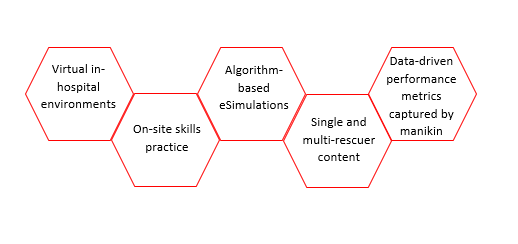
Valid Assessment, a systematic method of obtaining information used to draw inferences about characteristics.5
RQI Design Elements
Lauren Sanderson, MS, is the Cognitive Research Director at RQI Partners, LLC.
References
- Cheng A, Nadkarni VM, Mancini MB, et al; for the American Heart Association Education Science Investigators; and for the American Heart Association Education Science and Programs Committee, Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Cardiovascular and Stroke Nursing; and Council on Quality of Care and Outcomes Research. Resuscitation education science: educational strategies to improve outcomes from cardiac arrest: a scientific statement from the American Heart Association [published online ahead of print June 21, 2018]. Circulation. doi:10.1161/CIR.0000000000000583.
- Ericsson KA, Krampe RT, Tesch-Romer. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100:363–406. doi: 10.1037/0033-295X.100.3.363
- Van de Ridder JM, Stokking KM, McGaghie WC, ten Cate OT. What is feedback in clinical education? Med Educ. 2008;42:189–197. doi: 10.1111/j.1365-2923.2007.02973.x.
- Raemer D, Anderson M, Cheng A, Fanning R, Nadkarni V, Savoldelli G. Research regarding debriefing as part of the learning process. Simul Healthc. 2011;6(suppl):S52–S57. doi: 10.1097/SIH.0b013e31822724d0
- American Educational Research Association, American Psychological Association, National Council on Measurement in Education. The Standards for Educational and Psychological Testing. Washington, DC: American Education Research Association; 2014.241a.


{kind=link}